

Disaster or Opportunity: The Possible Effects of the USA New Order on Global Health in Nigeria
Explore the potential impact of the USA's withdrawal from the WHO on Nigeria's health sector. Learn about funding gaps, disease control disruptions and opportunities for adaptation and resilience.

Using Google’s Notebook’s LLM, this article has been repurposed into podcast form to help consume in an alternative. Please listen while you read along and let me know what you think!
Scarcely had the ink dried on the inauguration of President Donald Trump when he signed three executive orders—one of which withdrew the United States from the World Health Organization (WHO). This decision positioned the United States of America (USA) as the only nation, apart from Liechtenstein, to be a United Nations (UN) member but not part of the World Health Organisation (WHO).
While this move has sparked significant global controversy across the sociopolitical spectrum, its real-world implications are profound. Coupled with another Executive Order pausing international aid for 90 days pending review by the U.S. Budget Management Office, it has left public health experts and concerned citizens in developing countries alarmed. These regions rely heavily on multilateral agencies for funding and implementing critical health programs and initiatives.
Background
In his first week in office, President Donald Trump signed twenty one executive orders - three of which directly and indirectly impact global health.
“Withdrawing the United States from the World Health Organization” (Jan. 20) This order begins the process of withdrawing from the World Health Organization, or WHO. It also rescinds a prior executive order, signed by former President Joe Biden, that coordinated the federal government’s COVID-19 response efforts and implemented processes to respond to emerging pandemics.
“Reevaluating and Realigning United States Foreign Aid” (Jan. 20) This executive order immediately placed a 90-day pause on foreign aid or assistance to U.S. allies while the administration evaluates current aid programs. During this time, agencies will determine whether to resume, modify or cease foreign assistance programs at the end of the freeze.
“America First Policy Directive to the Secretary of State” (Jan. 20) This order directs the secretary of state to issue State Department guidance advancing “America First” foreign policy through the agency’s policies, programs, personnel and operations. The directive cites the need for championing the interests of American citizens above all else.
Source: NPR
USA’s Contributions to WHO and Global Health in Nigeria
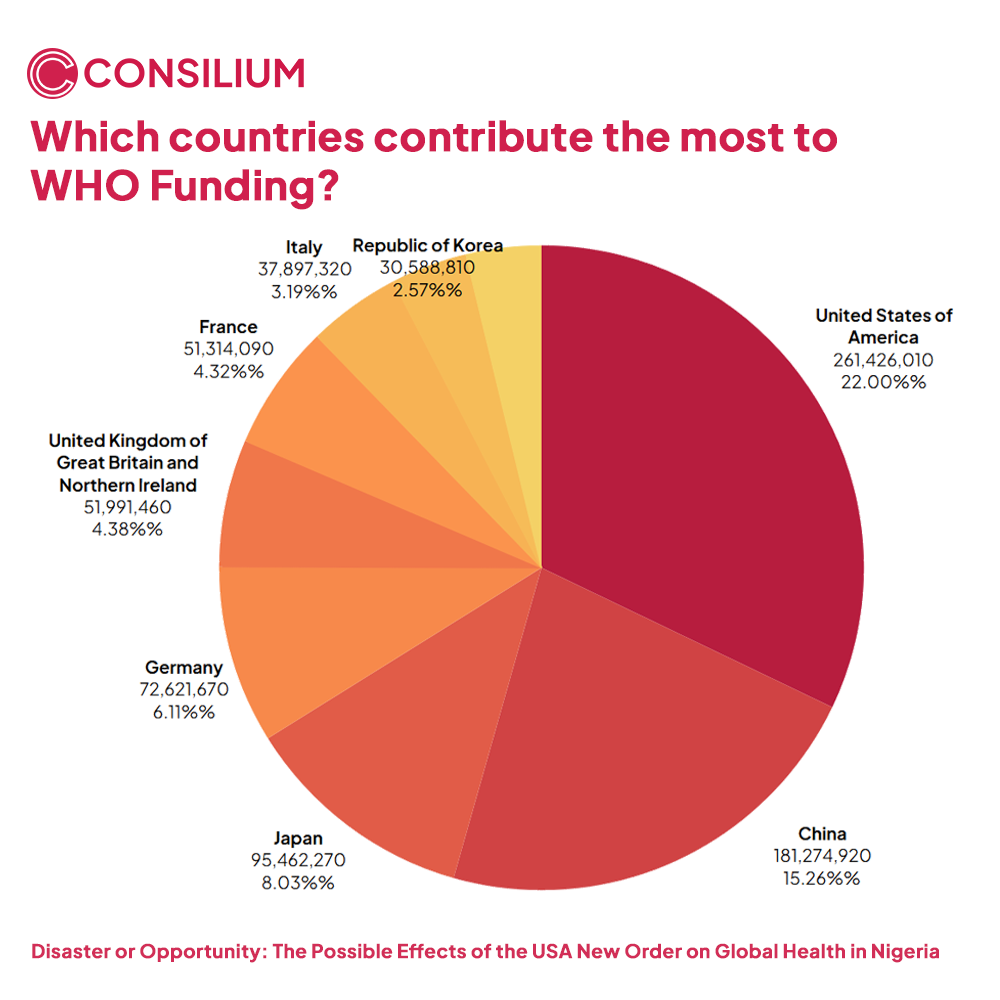
A founding member of the WHO, the United States remains its largest funder, with a net "compulsory" contribution of over $260 million budgeted for the 2025–2026 cycle. This is more than $85 million higher than the next largest contributor, China, which contributes $175 million. When voluntary contributions and contingency funds for emergencies are factored in, the U.S. contribution balloons to approximately $1.1 billion—nearly 20% of the WHO’s total budget. While this amount may seem modest compared to the U.S. Centers for Disease Control and Prevention (CDC) budget (less than one-third), its impact on the WHO’s operations is immense.
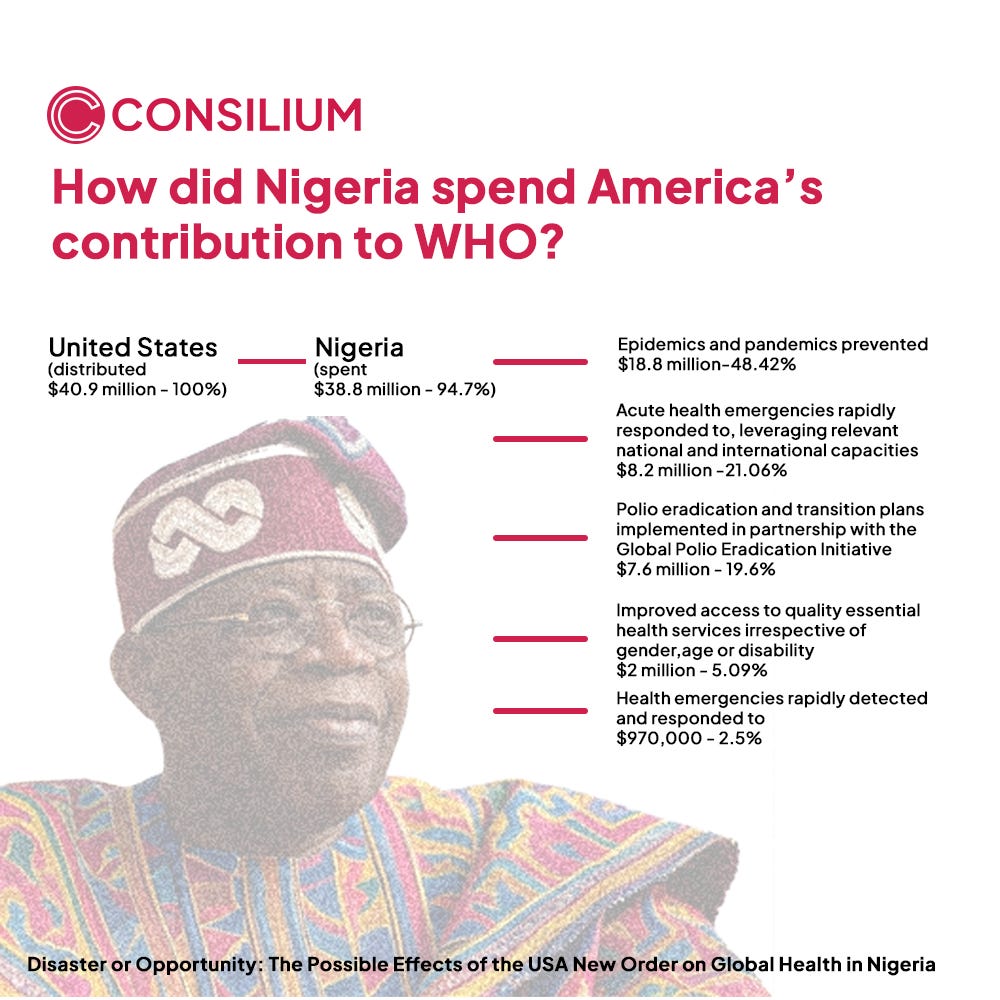
In 2023, Nigeria received $40 million in funding from the USA via the WHO. Nearly half of this funding (48.42%) was dedicated to preventing the spread of infectious diseases and managing public health risks. This significantly improved Nigeria's capacity for outbreak preparedness and response, aiding efforts to manage diseases like cholera, Lassa fever, and COVID-19. A substantial portion (21.06%) was allocated to rapid emergency responses, ensuring timely interventions during crises such as natural disasters or disease outbreaks. Additionally, almost one-fifth (19.6%) of the funding supported Nigeria’s polio eradication efforts, particularly through partnerships with the Global Polio Eradication Initiative, which was instrumental in Nigeria achieving its polio-free status in recent years.
Beyond WHO-directed funding, the USA's foreign aid policy—largely through the CDC and USAID—directly finances and implements several programs in Nigeria. These initiatives have had an immeasurable impact on strengthening the country’s health system. Examples include, but are not limited to:
U.S. President’s Malaria Initiative (PMI): Contributing to the fight against malaria since 2011, the PMI spent over $73 million in 2023 and has contributed a cumulative amount of over $900 million in eradicating malaria in Nigeria. This has touched over 120,000 homes, contributing to a 16% decrease in under-5 mortality in Nigeria while distributing 90 million mosquito nets and 115 million Rapid Diagnostic Test kits for free since the programme was established.
U.S. President’s Emergency Plan for AIDS Relief (PEPFAR): Perhaps the most popular programme on this list, PEPFAR has invested more than $6 billion in the Nigerian HIV/AIDS response. PEPFAR Nigeria is the third-largest programme globally and has touched over 2 million Nigerian men, women and children who are on ART treatment for free, a regimen which used to cost as high as $350. Beyond the financing, PEPFAR has laid a logistical and infrastructural framework which allows free testing, counselling, pharmaceutical warehousing and policy development towards the “95-95-95” goal of 2030.
Global Fund to Fight AIDS, Tuberculosis, and Malaria: GFATM was created by the Bill and Melinda Gates Foundation to eradicate HIV/AIDS, TB and malaria worldwide. With the highest incidence of TB and malaria on the African continent, Nigeria is one of the highest beneficiaries of the USA’s largesse as the highest donor ($26.31 billion) to this programme.
Integrated Health Program (IHP): The USAID Integrated Health Program (IHP) is a five- to seven-year, $225 million initiative aimed at reducing maternal and child morbidity and mortality in Nigeria by strengthening public and private health systems to support quality primary healthcare services. Operating in Bauchi, Kebbi, Ebonyi, Sokoto states, and the Federal Capital Territory (FCT), IHP has made significant strides in expanding health insurance coverage, improving routine immunization and COVID-19 vaccination efforts, and enhancing malaria diagnostic accuracy.
Nigeria Field Epidemiology and Laboratory Training Program (NFELTP): With technical and financial support from the U.S. Centers for Disease Control and Prevention (CDC), The Nigeria Field Epidemiology and Laboratory Training Program (NFELTP) is a workforce development initiative that has trained over 1,500 epidemiologists, equipping the Nigerian labour force to deal with public health crises.
Potential Direct Effects on Public Health in Nigeria
Funding Gaps
A significant consequence of funding cuts to WHO programs is the downstream scaling back of initiatives in Nigeria. This could halt and even reverse years of progress in eradicating diseases like polio and malaria. Such reductions in program scope would directly impact service delivery and health outcomes, particularly for vulnerable populations. Cuts could weaken disease surveillance systems, delay emergency response mechanisms, and increase the prevalence of preventable illnesses. Vulnerable groups, especially in underserved regions, would face heightened risks, undoing gains achieved over decades.
Disruption of Disease Control Efforts
Critical initiatives supported by the WHO, such as malaria elimination campaigns, immunization programs, and epidemic preparedness, are at risk of severe disruptions. Routine immunizations that protect millions of Nigerian children from vaccine-preventable diseases may be scaled back due to resource constraints. Malaria, which has seen significant control efforts, could resurge, particularly in the underserved northern regions. Even more concerning is the potential reversal of progress made by PEPFAR in reducing Nigeria's HIV/AIDS burden. Free antiretroviral therapy, interventions targeting mother-to-child transmission, and pre-/post-exposure prophylaxis programs may face setbacks, threatening the health of thousands of individuals.
Impact on Emergency Preparedness and Response
While Nigeria has made notable strides in emergency preparedness and response, funding cuts to developmental aid could undermine these gains. Reduced resources would likely impair the mobilization of human resources, diagnostic testing capacity, and disease surveillance systems, thus putting us at a higher risk of epidemic outbreak. This is especially critical in light of recent outbreaks such as anthrax in northern Nigeria and monkeypox. Cuts to WHO funding would also diminish its ability to coordinate multinational disease responses and provide technical support. The ultimate consequence would disproportionately impact marginalized and low-income populations.
Beyond all of the numbers, theories and facts, our improvement in healthcare indices in the Northern part of Nigeria has largely been as a result of foreign aid. Maternal mortality, malnutrition and availability of primary care services have all largely improved as a result of initiatives like the Integrated Health Programme. For the Amina and Musa on the streets of Kano, termination of funding goes beyond the “left” or “right” divide and instead is the line between life and death.
Indirect Effects on Nigeria’s Health Syste
m
Strain on Nigeria’s Health Financing
Beyond the political implication of the USA’s increasingly isolationist perspective to global policy, the onus of this systemic failure squarely rests at the feet of the Nigerian leadership. Successive Nigerian governments have failed at tackling health challenges which have plagued Nigeria since inception, instead outsourcing the moral, financial and technical obligations of implementing vertical and horizontal health programmes to international organisations, philanthropic organisations and foreign governments. This has morphed into an unfortunate situation where vast swathes of healthcare in Northern Nigeria solely depend on this for bare functionality.
Given the background context of the recent currency devaluation, inflation and the recurrent failure of the Nigerian government to meet the 15% benchmark allocation to health in the National budget, the Nigerian government is highly unlikely to be able to fund these programmes, leading to severe economic implications for an already underfunded health system.
Loss of Technical Expertise
While technical staff directly employed by the WHO are likely to remain in Nigeria, people who are directly employed by primarily-US agencies and are simply working on WHO-afiliated projects may have to return to their bases. This exodus of skilled personnel could lead to a significant gap in expertise, particularly in areas requiring specialized knowledge, such as disease surveillance, outbreak response, and program management. The loss of these professionals may also hinder the transfer of technical skills to local counterparts, weakening the long-term capacity of Nigeria’s health system to manage public health challenges independently
Opportunities for Adaptation
It is important to note that this is a temporary pause, not a permanent cessation of all USAID funding. It is in fact very likely that USAID funding in Nigeria is approved before the 90-day benchmark. However, The African Union’s Africa CDC (Africa Centres for Disease Control and Prevention) is a unique opportunity for African nations, including Nigeria, to bolster their collective capacity to address health emergencies. By pooling resources and expertise, the Africa CDC has the potential to fill critical gaps left by reduced WHO support. Leveraging Africa CDC’s networks, Nigeria can also coordinate more effective responses to cross-border health challenges, such as infectious disease outbreaks, which require swift, collaborative action.
Conclusion
As funding uncertainties from the WHO loom, Nigeria must explore alternative financing options to sustain its health programs. One viable approach is forming strategic partnerships with other global stakeholders such as the European Union (EU) and China. The EU has consistently supported global health initiatives and could provide supplementary funding for critical health interventions in Nigeria. Similarly, China, with its growing influence in Africa, has demonstrated an interest in health investments through infrastructure projects and medical aid. However, the lackadaisical attitude of the Nigerian government to health, considering recent occurrences like the COVID-19 pandemic does not inspire much belief in its readiness to bridge the gap.
For Nigeria and much of the Global South, the implications of the United States’ withdrawal from the World Health Organization extend far beyond the political theatrics of executive orders and threaten to unravel decades of progress in public health, from disease eradication to emergency preparedness. Lives and futures are at risk, with these consequences potentially able to topple an already-weak health system.
Nigeria needs to wake up.